
 |
| Image from Maxxl2 – Wikimedia Commons |
|

Author:
Fernando Pellerano, MS-V Universidad Iberoamericana (UNIBE) School of Medicine
Chemical eye injuries can occur from any exogenous material contacting the eye. This includes alkalis (e.g., lye, cements, plasters, airbag powder, bleach, and ammonia), acids (e.g., battery acid, pool cleaner, and vinegar), solvents, detergents, and irritants (e.g., mace).[2] Severity of the eye injury depends on the pH, concentration, and the nature of the chemical.
Acid injury is mainly a superficial disease, as coagulative necrosis occurs (precipitation of tissue protein), which prevents further penetration of chemical beyond the cornea. [3] One exception to this is hydrofluoric acid, which may rapidly pass through cell membranes and enter anterior chamber of the eye.[1]
Alkali injury is more common and more detrimental than injury from an acid. It causes a disruptive liquefactive necrosis with breakdown of normal cellular barriers, facilitating deeper penetration of chemicals into the anterior chamber, causing cataract formation and damage to the ciliary body and to the trabecular meshwork.[3] Patients usually describe a splash of chemical followed by moderate to severe pain, photophobia, blurred vision, and sensation of a foreign body. Reflex blepharospasm and red eye are common signs of chemical injury. If the affected eye looks white after exposure to an alkali (See Image A), it could be an indication of a particularly severe eye injury with ischemia of the conjunctival and scleral vessels.[4] A simple method of classifying the severity of chemical injury is the Roper – Hall Classification (See Table I).[3]
Examination should be systematic and include visual acuity, conjunctival examination for redness or blanching, an assessment of limbal vessel loss, fornix examination (including areas of conjunctiva between the lids and the globe for injury and residual chemical), assessment of the corneal epithelium and stroma, measurement of the IOP (Intra Ocular Pressure) and assessment of the anterior chamber for inflammation.[2]
Performing a thorough ophthalmic examination is crucial, but to increase chances of better prognosis, always remember this general Golden Rule:
Chemical injury is the only eye emergency in which treatment should not be delayed to evaluate visual acuity.
For immediate initial management, emergency physicians should follow these basic steps and tips:
- Keep the patient NPO in the event that surgery is required.
- The pH should be tested with graduated litmus paper to check for deviation from normal eye pH (7.0-7.4). [3]
- Initiate copious but gentle irrigation using saline or Ringer’s lactate solution for at least 30 minutes as soon as injury from a chemical is suspected. Tap water can be used in the absence of these solutions. [2]
- Consider discussion with an ophthalmologist once you have started irrigation.
- Topical anesthetics (e.g., tetracaine) help to relieve pain and thus facilitate eye irrigation. The eye can be irrigated using an intravenous tube, nasal cannula, or Morgan lens (See Image B).[4]
- NEVER use acidic solutions to neutralize alkalis or vice-versa, as acid–base reactions themselves can generate harmful substances. [2]
- Wait 5 to 10 minutes after irrigation is stopped to allow the dilutant to be absorbed, then check the pH in the fornices (the area between the eyelid and globe) using litmus paper. Irrigation is continued until neutral pH is achieved and maintained for 30 minutes. [2] The volume required for irrigation may range from 2 to 10 liters. [4]
- Conjunctival fornices should be swept with a moistened cotton-tipped applicator or glass rod to remove any sequestered particles of caustic material and necrotic conjunctiva, especially in the case of a persistently abnormal pH. [2]
- Once pH is stabilized, a broad-spectrum topical antibiotic (Ciprofloxacin, Ofloxacin, Gentamicin, or Tobramycin) should be applied and acetaminophen or opioids should be used for pain control. A cycloplegic agent may also be considered [4]
- If you get a call about an eye injury you may instruct the patient to bring the chemical, if possible. It may be helpful to find out the exact chemical used.
Overall, when talking about ocular chemical burns the first and foremost interventions are irrigation, irrigation and irrigation.
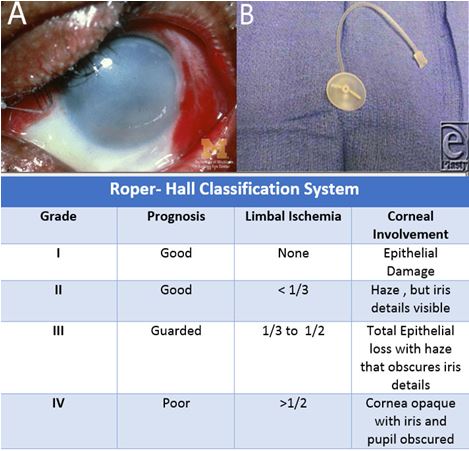
(A) Cornea opacified by an alkali burn.
(B) Morgan Lens.
(Table I) The Roper- Hall Classification of chemical injury.
Image A available at http://www.kellogg.umich.edu/theeyeshaveit/trauma/chemical-burn.html “Chemical Burn” created by Jonathan Trobe, M.D, University of Michigan Kellogg Eye and The Reagents of the University of Michigan, used under Creative Commons Attribution license.
Image B is available at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3230139/ “Chemical Burn to the Eye” by Justin Klaff, MD, Stephen M Milner, BDS, FRCS (Ed), FACS, Stuart Farris, MD, and Leigh Ann Price, MD in Eplasty (Open Acces Journal of Plastic Surgery), used under Creative Commons Attribution license.
Table I is adapted from Roper Hall MJ. Thermal and Chemical Burns. Trans Ophthalmol Soc UK 1965; 85:631-53.
- Singh P, Tyagi M, Kumar Y, Gupta K, Sharma P.D. Ocular Chemical Injuries and their Management. Oman J Ophthalmol. 2013; 6(2): 83–86. PMID: 24082664
- Gerstenblith A, Rabinowitz M. Trauma: Chemical Burn In Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2012.
- Borooah S, Wright M, Dhillon B. Chemical Injury In Ophthalmology Pocket Tutor.1st ed. London, UK: JP Medical Ltd; 2012.
- Pokhrel P, Loftus S. Ocular Emergencies. Am Fam Physician. 2007; 76(6) 829-836. PMID: 17910297