
 |
||
Image Credit: Image from James Heilman, MD
|

Author: Jeffrey Chen, MSIII
University of California San Francisco
Case: A previously healthy 18-year-old male comes in to the pediatric emergency department complaining of severe bilateral soreness and weakness of quadriceps and dark tea-colored urine for 1 day. Yesterday at the gym he performed heavy squats and lunges consecutively for one hour and drank minimal water. He denies recent URI symptoms or trauma.
Vitals are within normal limits. On exam, the patient’s anterior thighs are hard, swollen, and tender to touch and have limited passive and active range of motion. Sensation and capillary refill are normal in the distal lower extremities. Serum creatine kinase levels are 41,000; other labs include: BUN 14, Creatinine 0.73, Potassium 4.4, Phosphorus 3.8, Calcium 8.8. Urine dipstick is positive for blood, though no RBCs are seen on microscopy. MRI imaging shows edema and inflammation of the anterior compartment of the thighs, with patent blood vessels and no evidence of nerve damage (see image 1).
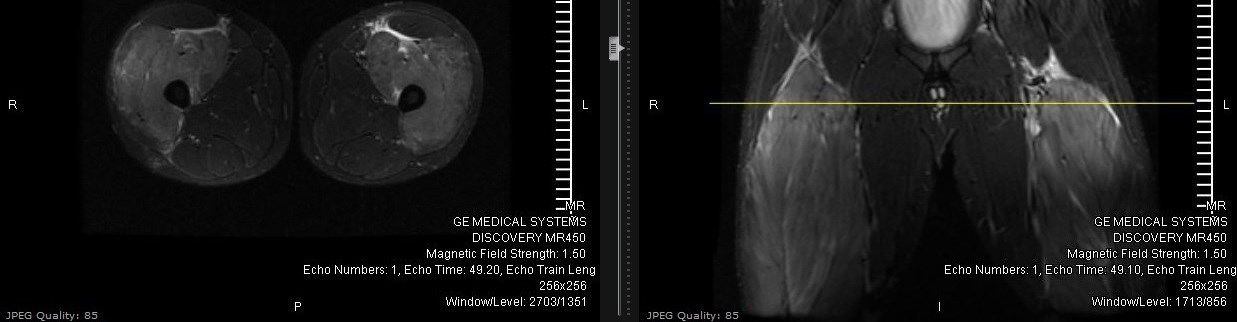 |
| Image 1 |
Pathophysiology/Complications:
Rhabdomyolysis occurs when muscle fibers break down, releasing a flood of internal contents into the bloodstream.[1-4] These changes lead to abnormalities in:
- Creatine kinase: used as a serum marker to diagnose and trend the clinical course; levels >5x reference range (generally >1500 IU/L) suggest this diagnosis
- Myoglobin: can precipitate in kidneys and cause obstructive renal failure; forms ferrihemate at low filtrate pH, which is directly nephrotoxic
- Potassium: released from damaged muscle cells; hyperkalemia can reach cardiotoxic levels if not managed
- Phosphate: also released from cells, leading to hyperphosphatemia
- Uric acid: released from cells, leading to hyperuricemia
- Calcium: deposits in damaged cells, leading to hypocalcemia
- Thromboplastin: can rarely lead to DIC
Careful monitoring of these proteins and electrolytes is crucial in preventing complications such as acute kidney injury or cardiac arrhythmias. Reversible hepatic injury also occurs in ~25% of patients, though the specific mechanism is unclear. Third spacing of fluid into injured muscle can lead to hypovolemia, which can exacerbate acute kidney injury (AKI), as well as compartment syndrome if swollen fibers go on to compress nerves and blood vessels.
Epidemiology/Prognosis:
At least 26,000 cases of rhabdomyolysis are documented each year in the US, affecting more adults than children. The rate of myoglobin-induced AKI varies in different studies, ranging from 15-45%.[5] About a third of patients go on to require dialysis, and overall mortality with rhabdomyolysis remains about 5%.[6]
Etiologies:
The majority of cases in adults are caused by trauma and muscle overexertion, which can be exacerbated by dehydration, extreme temperatures, drug use, and lack of regular training.[7] Crush injuries or prolonged stasis can also lead to rhabdomyolysis. Rarer causes include infections (most commonly Legionella), statins/fibrates, and drug use (cocaine, meth, heroin). In children, the leading causes are viral infections (commonly influenza), which typically present as URI/fever symptoms 1-14 days before the onset of rhabdomyolysis.[8] Trauma is responsible for 26% of cases in children. Even rarer causes in all age groups include consuming buffalo fish (Haff disease), hemlock herbs, or quail, and exposure to snake/spider venom.[9]
Workup:
The classic triad of rhabdomyolysis is muscle soreness, weakness, and dark urine, accompanied by a history of a potential cause.[2] Physical exam may reveal muscle swelling, tenderness, and decreased range of motion. Compartment syndrome should be ruled out. A urine dipstick is positive for blood in ~50% due to the myoglobin but will be negative on microscopy for RBCs. Lab tests to be ordered include CBC, CMP, coags, creatine kinase, and phosphate levels. X-rays and MRIs should be considered to screen for fractures in trauma and for compartment syndrome.[10]
Management:
Much like “golden hour” for trauma, there is a “golden 6 hours” for time to treatment of rhabdomyolysis to prevent the development of severe AKI.[11] The mainstay of management is aggressive IV hydration. Start with at least 1-2 liter boluses of normal saline in the emergency department, depending on the patient’s volume status. Then begin aggressive maintenance fluid hydration (e.g., 2x maintenance) with a goal urine output of 200 mL per hour (or 3 mL/kg/hr). The objective is to aggressively flush myoglobin out of the kidneys until CK levels reach <10,000 (some sources say <5,000). Alkalinizing the urine with sodium bicarbonate to a urine pH >6.5 limits the precipitation of myoglobin and the formation of toxic ferrihemate in the kidneys. Electrolytes should be continuously monitored and any abnormalities corrected. Hemodialysis may be considered for severe electrolyte abnormalities (such as hyperkalemia) unresponsive to medical management. Additionally, serial physical exams should be performed to detect the development of compartment syndrome.
Case Continued:
This young patient with exertional rhabdomyolysis was admitted to the inpatient pediatric unit, where aggressive IV hydration and urine alkalinization prevented AKI from ever developing, with creatinine ranging from 0.67 to 0.77. CK peaked at 330,276 on day 2 of hospitalization and steadily went down over the hospital course. The patient walked out of the hospital 8 days after initial presentation, promising to drink plenty of fluids at his next work out.
References:
1. Bosch et al. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009 Jul 2;361(1):62-7
2. Luck RP, Verbin S. Rhabdomyolysis: a review of clinical presentation, etiology, diagnosis, and management.Pediatr Emerg Care. 2008 Apr. 24(4):262-8.
3. Ward MM. Factors predictive of acute renal failure in rhabdomyolysis. Arch Intern Med. 1988 Jul. 148(7):1553-7.
4. Vanholder R, Sever MS, Erek E, Lameire N. Rhabdomyolysis. J Am Soc Nephrol. 2000 Aug. 11(8):1553-61.
5. Wu CT, Huang JL, Lin JJ, Hsia SH. Factors associated with nontraumatic rhabdomyolysis and acute renal failure of children in Taiwan population. Pediatr Emerg Care. 2009 Oct. 25(10):657-60.
6. Mannix R, Tan ML, Wright R, Baskin M. Acute pediatric rhabdomyolysis: causes and rates of renal failure.Pediatrics. 2006 Nov. 118(5):2119-25.
7. Huerta-Alardín AL, Varon J, Marik PE. Bench-to-bedside review: Rhabdomyolysis — an overview for clinicians. Crit Care. 2005 Apr. 9(2):158-69.
8. Nauss MD, Schmidt EL, Pancioli AM. Viral myositis leading to rhabdomyolysis: a case report and literature review. Am J Emerg Med. 2009 Mar. 27(3):372.e5-372.e6.
9. Herman LL, Bies C. Haff Disease: Rhabdomyolysis After Eating Buffalo Fish. Western J Emerg Med. 2014;15(6):664-666.
10. Moratalla MB, Braun P, Fornas GM. Importance of MRI in the diagnosis and treatment of rhabdomyolysis. Eur J Radiol. 2008 Feb. 65(2):311-5.
11. Sinert R, Kohl L, Rainone T, Scalea T. Exercise-induced rhabdomyolysis. Ann Emerg Med. 1994;23:1301–6.