
 |
| Image – Bigstock |
Author: Jake Toy, OMS II
Western University of Health Sciences
College of Osteopathic Medicine of the Pacific, Pomona, CA
AAEM/RSA Publications Committee Member
 |
| This post was peer reviewed. Click to learn more. |
Introduction
There are an estimated 424,000 out of hospital cardiac arrests (OHCA) among Americans annually.[1] Survival rates for OHCA are low, ranging from 10.6% to 31.4%.[2] External defibrillation and CPR represent the first line treatments for OHCA. The American Heart Association (AHA) defines high-quality CPR as 100-120 compressions per minute (CPM) at a depth of 2 inches on the average adult. Allowance of full recoil, minimization of compression interruptions, and avoidance of excessive ventilation are also important (Figure 1).[3]
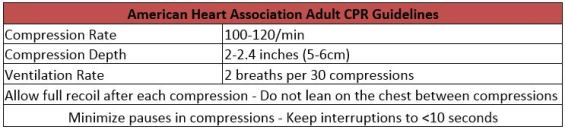 |
| Figure 1. 2015 American Heart Association Adult CPR Guidelines (Source – American Heart Association[2]) |
Clinical studies have shown that the quality of CPR performed by EMS providers for OHCA often does not meet AHA standards.[4-6] Previous studies have found that a depth of <1.5 inches was delivered 37.4% to 72% of the time during resuscitation efforts. Compression rates were <80/min during 36.9% of 30-second time segments during CPR and <70/min during 21.7% of time segments.[4-8] It is important to note suboptimal performances in depth and rate are directly correlated with adverse patient outcomes and survival.[4-7, 9]
Additionally, interruptions during CPR can significantly decrease patient survival rates. A key goal in the attempt to re-establish organ perfusion is the maintenance of coronary perfusion pressure (CPP) >15mmHg. CPP is a primary predictor for a return of spontaneous circulation (ROSC) and survival.[6, 9]
Whether it is an interruption during transport or prior to defibrillation, any pause, even if only for few a seconds, immediately disrupts myocardial perfusion, CPP levels, and carotid artery flow.[8, 10-12] Restoration of circulation after a pause in CPR takes approximately 10 seconds, however, it may take over 90 seconds to restore CPP to appropriate levels.[12] Further, studies have shown that decreasing the pre-shock pause in CPR by just five seconds can increase the odds of shock success by 86% in patients in ventricular fibrillation.[11] As such, CPR interruption time strongly correlates with patient survival.
Mechanical CPR presents a potential solution to the CPR interruptions and compression depth and rate inconsistencies that are associated with manual CPR. The two most widely utilized mechanical devices are the Lund University Cardiac Arrest System (LUCAS) (Physio Control/Jolife AB, Lund, Sweden) and the AutoPulse Device (ZollMedical, Chelmsford, MA, USA). Between 2007 to 2011, the United States witnessed a 1,511% increase in the utilization of mechanical CPR devices such as these.[13] Both are portable devices that can be operated on scene and during transport to provide automatic chest compressions.
LUCAS (Piston CPR device)
The LUCAS-1 was introduced in Europe in 2006. A silicone rubber suction cup mounted on two legs was attached to a pneumatic cylinder that provided active compressions and decompressions.[14] The device was powered by an external supply of oxygen or air. This unit was replaced in 2009 by the LUCAS-2, a battery powered unit, which eliminates the gas powered cylinder.[15] With the LUCAS systems, force is primarily concentrated on the sternum.
 |
| Figure 2. Left) LUCAS-2 Right) LUCAS-2 employs piston driven CPR with force focused on a patient’s sternum (Source – physiocontrol.com[16]) |
AutoPulse (Load Distributing Band Device)
The AutoPulse device consists of a load-distributing band (LDB) attached to a backboard. Powered by a motor in the backboard, the band tightens and loosens to provide compressions.[17] The LDB distributes force over the sternum and rib cage.
 |
| Figure 3. AutoPulse device deployed on a mannequin. (Image from Wikimedia Commons – PhilippN ) |
Mechanical CPR verse Manual CPR
Studies comparing the LUCAS and AutoPulse devices in animal experiments revealed promising results. Both devices were shown to increase hemodynamic flow, as well as improve cerebral perfusion, cardiac output, and myocardial perfusion in experimental animals when compared to manual CPR.[14, 18, 19]
These initially promising results, however, were not mirrored in improved patient outcomes during subsequent clinical trials (Table 1). In 2014, LUCAS-1 CPR with simultaneous defibrillation was compared to manual CPR in the LINC Randomized Trial. This trial evaluated 2,589 OHCA patients in Western Europe. When comparing 4hr survival between the LUCAS-1 and manual CPR, the LUCAS-1 was not superior to manual CPR (23.6% vs. 23.7% respectively).[20] In 2015, the LUCAS-2 was evaluated in the PARAMEDIC trial. This study evaluated 4,471 OHCA patients in the UK who were administered manual CPR or LUCAS-2 CPR. This study found no improvement in 30-day survival when utilizing the LUCAS-2.[21]
In 2006, the AutoPulse device was evaluated. One study assessed ROSC in OHCA patients who received LDB-CPR or manual CPR in Richmond, VA. A total of 499 OHCA patients received manual CPR and 284 received LDB-CPR. Of patients receiving manual CPR, 20.2% achieved ROSC compared to 34.5% in the LDB-CPR group. Results indicated that LDB-CPR appeared to increase incidence of ROSC.[17] Another study assessed 4hr survival of patients who received LDB-CPR versus manual CPR. Preliminary results showed that LDB-CPR, as implemented in this study, worsened patient survival. The study was terminated early due to safety concerns.[22]
In 2014, the AutoPulse device was evaluated by the CIRC study. It involved 4,231 patients, from the USA and Europe. This study concluded that there was equivalent survival between LDB-CPR and manual CPR.[23]
Of note, no changes in neurological outcome nor an increase in the risk of injury was found between mechanical CPR and manual CPR groups in any of the studies described.[17, 20-25]
 |
|
PO = primary outcome, SO = secondary outcome
Table 1. Clinical studies assessing the LUCAS and AutoPulse devices |
Mechanical CPR – a practical evaluation
There are some important practical advantages and disadvantages of mechanical CPR, other than the question of effect on clinical outcomes.
Advantages of Mechanical CPR
- Reduces inconsistencies in depth and rate, especially during transport or when inexperienced providers administer CPR.[5, 6, 8, 11, 26]
- Decreases interruption time and enables rescuers to deliver a simultaneous shock during compressions.[11]
- Eliminates rescuer fatigue and frees up the hands and minds of personnel in situations of limited human resources, such as in rural areas or while transporting a cardiac arrest patient during ongoing CPR.[27]
- Is conceivably safer compared to manual CPR during ambulance transport, helicopter transport or mountain rescue operations where administration of manual CPR may be challenging.[28, 29]
Disadvantages of Mechanical CPR
- Device failure or malfunction with or without provider awareness.[26]
- Financial investment and initial training or support resources associated with implementation.
Conclusion
Currently, little clinical evidence suggests that mechanical CPR is superior to manual CPR. However, there are practical advantages to mechanical CPR that must be considered. Though it is unlikely that mechanical CPR will completely replace manual CPR, as technology advances, it appears plausible that mechanical CPR devices could one day surpass the capabilities of manual CPR.
Resources
1. Go A, Mozaffarian D, Roger V, et al. Heart Disease and Stroke Statistics—2014 Update. Circulation. 2014 Jan 21;129(3):28-292.
2. Mozaffarian D, Benjamin E, Go A, et al. Heart Disease and Stroke Statistics—2015 Update. Circulation. 2015 Jan 27;131(4):29-322.
3. Hazinski M, Shuster M, Donnino M, et al. Highlights of the 2015 American Heart Association Guidelines Update for CPR and ECC. In: Association AH, editor.; 2015.
4. Abella B, Sandbo N, Vassilatos P, et al. Chest compression rates during cardiopulmonary resuscitation are suboptimal: a prospective study during in-hospital cardiac arrest. Circulation. 2005;111(4):428-34.
5. Kramer-Johansen J, Myklebust H, Wik L, et al. Quality of out-of-hospital cardiopulmonary resuscitation with real time automated feedback: A prospective interventional study. 71. 2006;3:283-92.
6. Wik L, Kramer-Johansen J, Myklebust H, et al. Quality of cardiopulmonary resuscitation during out-of-hospital cardiac arrest. JAMA. 2005;293(3):299-304.
7. Abella B, Alvarado J, Myklebust H, et al. Quality of cardiopulmonary resuscitation during in-hospital cardiac arrest. JAMA. 2005;293(3):305-10.
8. Edelson D. The Science of CPR – Identifying the factors key to improved patient outcomes. JEMS. 2010.
9. Paradis N, Martin G, Rivers E, et al. Coronary perfusion pressure and the return of spontaneous circulation in human cardiopulmonary resuscitation. JAMA. 1990 Feb 13;263(8):1106-13.
10. Olasveengena T, Wik L, Steen P. Quality of cardiopulmonary resuscitation before and during transport in out-of-hospital cardiac arrest. Resuscitation. 2008;76(2):185-90.
11. Edelson D, Abella B, Kramer-Johansen J, et al. Effects of compression depth and pre-shock pauses predict defibrillation failure during cardiac arrest. Resuscitation. 2006;71(2):137-45.
12. Steen S, Liao Q, Pierre L, Paskevicius A, Sjoberg T. The critical importance of minimal delay between chest compressions and subsequent defibrillation: a haemodynamic explanation. Resuscitation. 2003;58(3):249-58.
13. Stretch R, Sauer C, Yuh D, Bonde P. National trends in the utilization of short-term mechanical circulatory support: incidence, outcomes, and cost analysis. J Am Coll Cardiol. 2014;64(14):1407-15.
14. Steen S, Liao Q, Pierre L, Paskevicius A, Sjöberg T. Evaluation of LUCAS, a new device for automatic mechanical compression and active decompression resuscitation. 2002;55(3):285-99.
15. Lucas – Chest Compression System. [cited 2015 Dec 21]; Available from: http://www.lucas-cpr.com
16. LUCAS 2 Chest Compression System. Physio-Control Inc.
17. Ong M, Ornato J, Edwards D, et al. Use of an automated, load-distributing band chest compression device for out-of-hospital cardiac arrest resuscitation. JAMA. 2006 Jun 14;295(22):2629-37.
18. Halperin H, Paradis N, Ornato J, et al. Cardiopulmonary resuscitation with a novel chest compression device in a porcine model of cardiac arrest: improved hemodynamics and mechanisms. J Am Coll Cardiol. 2004 Dec 7;44(11):2214-20.
19. Rubertsson S, Karlsten R. Increased cortical cerebral blood flow with LUCAS; a new device for mechanical chest compressions compared to standard external compressions during experimental cardiopulmonary resuscitation. Resuscitation. 2005 Jun;65(3):357-63.
20. Rubertsson S, Lindgren E, Smekal D, et al. Mechanical Chest Compressions and Simultaneous Defibrillation vs Conventional Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac Arrest The LINC Randomized Trial. JAMA. 2014;311(1):53-61.
21. Perkins G, Lall R, Quinn T, et al. Mechanical versus manual chest compression for out-of-hospital cardiac arrest (PARAMEDIC): a pragmatic, cluster randomised controlled trial. Lancet. 2015 Mar 14;385(9972):947-55.
22. Hallstrom A, Rea T, Sayre M, et al. Manual chest compression vs use of an automated chest compression device during resuscitation following out-of-hospital cardiac arrest: a randomized trial. JAMA. 2006;295(22):2620-8.
23. Wik L, Olsen J, Persse D, et al. Manual vs. integrated automatic load-distributing band CPR with equal survival after out of hospital cardiac arrest. The randomized CIRC trial. Resuscitation. 2014;85(6):741-8.
24. Prinzing A, Eichhorn S, Deutsch M, Lange R, Krane M. Cardiopulmonary resuscitation using electrically driven devices: a review. J Thorac Dis. 2015;7(10):459-67.
25. Bonnes JL, Brouwer MA, Navarese EP, et al. Manual Cardiopulmonary Resuscitation Versus CPR Including a Mechanical Chest Compression Device in Out-of-Hospital Cardiac Arrest: A Comprehensive Meta-analysis From Randomized and Observational Studies. Ann Emerg Med. 2016 Mar;67(3):349-60.e3.
26. Ong M, Mackey K, Zhang Z, et al. Mechanical CPR devices compared to manual CPR during out-of-hospital cardiac arrest and ambulance transport: a systematic review. Scand J Trauma Resusc Emerg Med. 2012;20(39).
27. Hightower D, Thomas S, Stone C, Dunn K, March J. Decay in quality of closed-chest compressions over time. Ann Emerg Med. 1995;26(3):300-3.
28. Gässler H, Kümmerle S, Ventzke M, Lampl L, Helm M. Mechanical chest compression: an alternative in helicopter emergency medical services? Intern Emerg Med. 2015;2015(10):6.
29. Pietsch U, Lischke V, Pietsch C. Benefit of mechanical chest compression devices in mountain HEMS: lessons learned from 1 year of experience and evaluation. Air Med J. 2014;33(6):299-301.